Fill a Valid De Ins Illinois Form
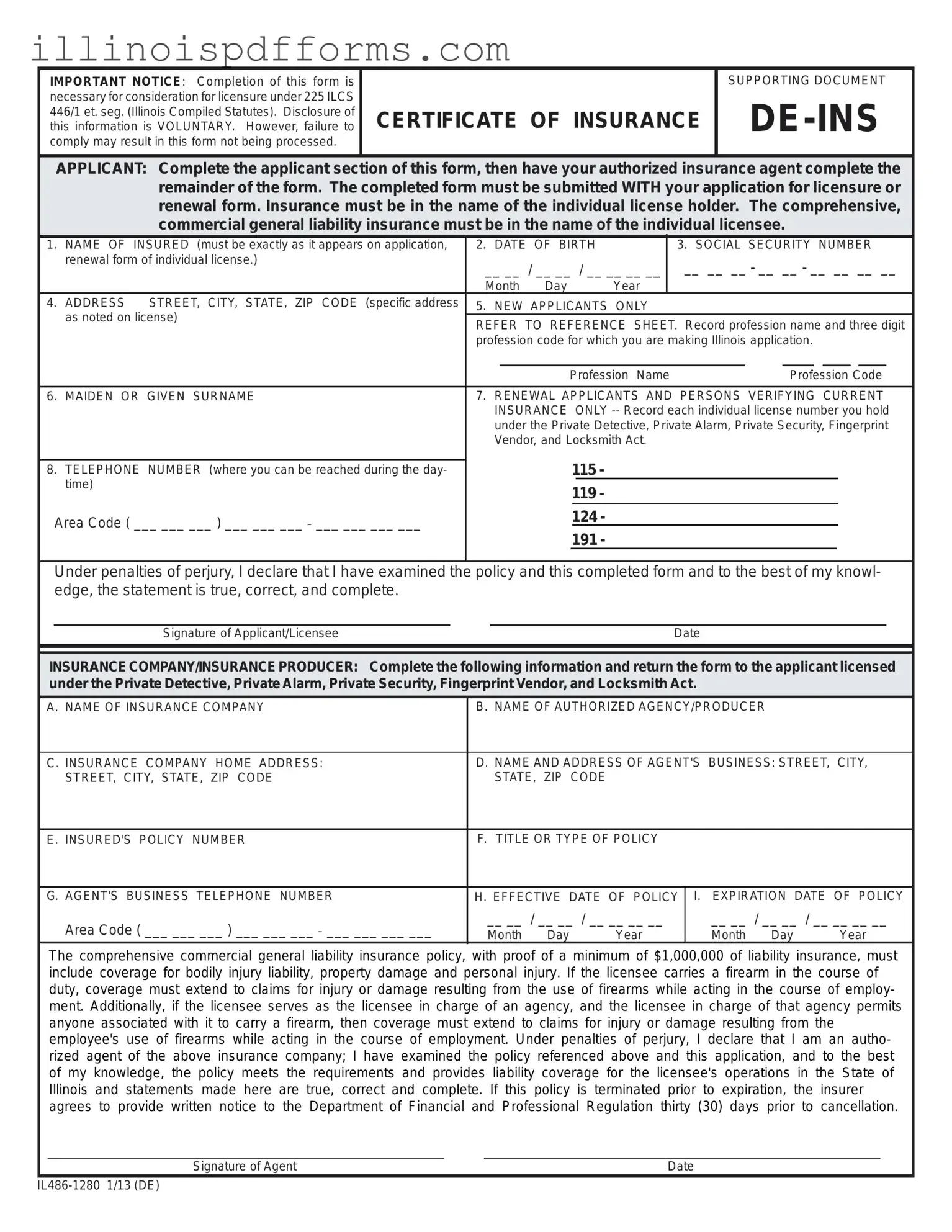
The De Ins Illinois form plays a crucial role in the licensure process for professionals operating under the Private Detective, Private Alarm, Private Security, Fingerprint Vendor, and Locksmith Act. This form must be completed accurately and submitted alongside the application for licensure or renewal. It requires specific information from the applicant, including their name, date of birth, and social security number, all of which must match the details on their application. The applicant must also provide their address and contact number. For new applicants, additional details such as the profession name and corresponding code are necessary. Insurance details are equally important; the form mandates that applicants secure comprehensive commercial general liability insurance, with a minimum coverage of $1,000,000. This insurance must be in the applicant's name and include coverage for bodily injury, property damage, and personal injury. If firearms are carried during the course of duty, the insurance must also cover related claims. The form must be signed by both the applicant and the authorized insurance agent, ensuring that all information is accurate and complete. Failure to comply with these requirements can lead to delays or rejection of the application.
Example - De Ins Illinois Form
IMPORTANT NOTICE: Completion of this form is |
|
SUPPORTING DOCUMENT |
necessary for consideration for licensure under 225 ILCS |
|
|
446/1 et. seg. (Illinois Compiled Statutes). Disclosure of |
CERTIFICATE OF INSURANCE |
|
this information is VOLUNTARY. However, failure to |
||
comply may result in this form not being processed. |
|
|
|
|
|
APPLICANT: Complete the applicant section of this form, then have your authorized insurance agent complete the remainder of the form. The completed form must be submitted WITH your application for licensure or renewal form. Insurance must be in the name of the individual license holder. The comprehensive, commercial general liability insurance must be in the name of the individual licensee.
1. |
NAME OF INSURED (must be exactly as it appears on application, |
2. |
DATE OF BIRTH |
|
3. SOCIAL SECURITY NUMBER |
||||||||||||
|
renewal form of individual license.) |
__ __ / __ __ / __ __ __ __ |
|
__ __ __ - __ __ - __ __ __ __ |
|||||||||||||
|
|
|
|||||||||||||||
|
|
Month Day |
|
|
Year |
|
|
|
|
|
|
|
|
|
|
||
4. |
ADDRESS STREET, CITY, STATE, ZIP CODE (specific address |
5. |
NEW APPLICANTS ONLY |
|
|
|
|
|
|
|
|
|
|||||
|
as noted on license) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REFER TO REFERENCE SHEET. Record profession name and three digit |
||||||||||||||||
|
|
||||||||||||||||
|
|
profession code for which you are making Illinois application. |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Profession Name |
|
|
Profession Code |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
6. |
MAIDEN OR GIVEN SURNAME |
7. RENEWAL APPLICANTS AND PERSONS VERIFYING CURRENT |
|||||||||||||||
|
|
|
INSURANCE |
|
ONLY |
||||||||||||
|
|
|
under the Private Detective, Private Alarm, Private Security, Fingerprint |
||||||||||||||
|
|
|
Vendor, and Locksmith Act. |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
115 - |
|
|
|
|
|
|
|
|
|
|
||
8. |
TELEPHONE NUMBER (where you can be reached during the day- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
time) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
119 - |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Area Code ( ___ ___ ___ ) ___ ___ ___ _ ___ ___ ___ ___ |
|
|
|
|
124 - |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
191 - |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Under penalties of perjury, I declare that I have examined the policy and this completed form and to the best of my knowl- edge, the statement is true, correct, and complete.
Signature of Applicant/LicenseeDate
INSURANCE COMPANY/INSURANCE PRODUCER: Complete the following information and return the form to the applicant licensed under the Private Detective, Private Alarm, Private Security, Fingerprint Vendor, and Locksmith Act.
A. NAME OF INSURANCE COMPANY |
B. NAME OF AUTHORIZED AGENCY/PRODUCER |
|
|||
|
|
|
|||
C. INSURANCE COMPANY HOME ADDRESS: |
D. NAME AND ADDRESS OF AGENT'S BUSINESS: STREET, CITY, |
||||
STREET, CITY, STATE, ZIP CODE |
STATE, ZIP CODE |
|
|
|
|
|
|
|
|
||
E. INSURED'S POLICY NUMBER |
F. TITLE OR TYPE OF POLICY |
|
|
||
|
|
|
|||
G. AGENT'S BUSINESS TELEPHONE NUMBER |
H. EFFECTIVE DATE OF POLICY |
I. EXPIRATION DATE OF POLICY |
|||
Area Code ( ___ ___ ___ ) ___ ___ ___ _ ___ ___ ___ ___ |
__ __ / __ __ / __ __ __ __ |
__ __ / __ __ / __ __ __ __ |
|||
Month Day |
Year |
Month Day |
Year |
||
|
|||||
The comprehensive commercial general liability insurance policy, with proof of a minimum of $1,000,000 of liability insurance, must include coverage for bodily injury liability, property damage and personal injury. If the licensee carries a firearm in the course of duty, coverage must extend to claims for injury or damage resulting from the use of firearms while acting in the course of employ- ment. Additionally, if the licensee serves as the licensee in charge of an agency, and the licensee in charge of that agency permits anyone associated with it to carry a firearm, then coverage must extend to claims for injury or damage resulting from the employee's use of firearms while acting in the course of employment. Under penalties of perjury, I declare that I am an autho- rized agent of the above insurance company; I have examined the policy referenced above and this application, and to the best of my knowledge, the policy meets the requirements and provides liability coverage for the licensee's operations in the State of Illinois and statements made here are true, correct and complete. If this policy is terminated prior to expiration, the insurer agrees to provide written notice to the Department of Financial and Professional Regulation thirty (30) days prior to cancellation.
Signature of Agent |
Date |
Document Breakdown
| Fact Name | Details |
|---|---|
| Governing Law | The De Ins Illinois form is governed by 225 ILCS 446/1 et. seq. of the Illinois Compiled Statutes. |
| Purpose | This form is a supporting document necessary for consideration for licensure in specific professions. |
| Voluntary Disclosure | Disclosure of information on this form is voluntary; however, non-compliance may result in processing delays. |
| Insurance Requirements | The form requires proof of comprehensive commercial general liability insurance with a minimum coverage of $1,000,000. |
| Submission Requirement | The completed form must be submitted along with the application for licensure or renewal. |
| Agent's Declaration | Agents must declare that the insurance policy meets the necessary requirements and provide coverage for the licensee's operations. |
Create More PDFs
Hfs 3654 - Filing this form accurately helps in reducing fraud and error rates in state healthcare spending.
Certificate of Registration Illinois - The form requires renewal every five years to ensure the Illinois Department of Revenue has current information on all self-assessing purchasers.