Fill a Valid Illinois Boa 4 Form
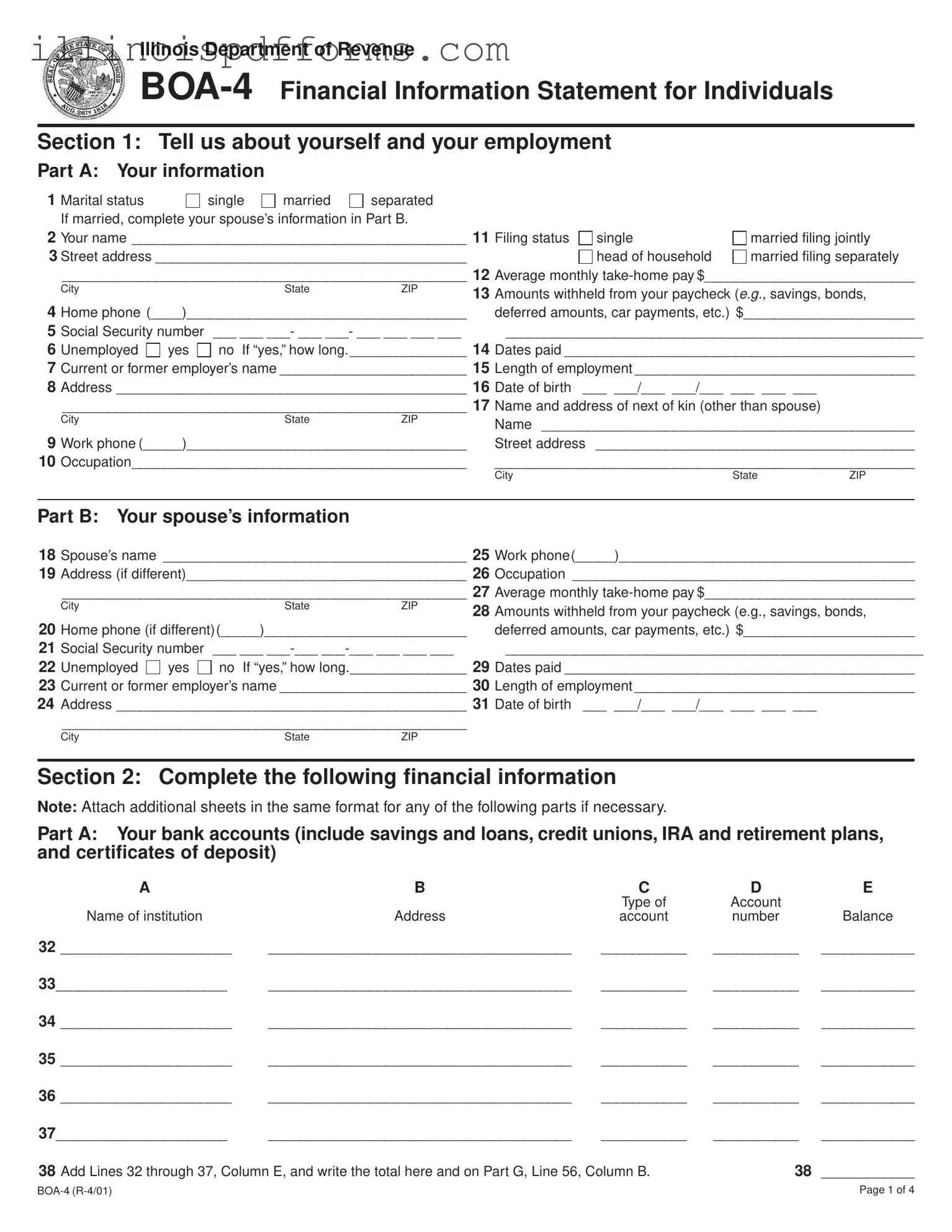
The Illinois BOA-4 form serves as a comprehensive Financial Information Statement designed for individuals to report their financial status to the Illinois Department of Revenue. This form is particularly relevant for those seeking assistance or adjustments regarding their tax obligations. It consists of several sections that require detailed personal and financial information. The first section gathers basic details about the individual, including marital status, employment information, and income sources. The second section delves deeper into the individual's financial assets, such as bank accounts, credit lines, real property, and insurance policies. Additionally, it requests information about liabilities, including debts and taxes owed. The final sections focus on analyzing monthly income and expenses, allowing individuals to provide a complete picture of their financial situation. By ensuring all relevant data is accurately reported, the BOA-4 form plays a crucial role in facilitating fair assessments and decisions regarding tax-related matters.
Example - Illinois Boa 4 Form
Illinois Department of Revenue
Section 1: Tell us about yourself and your employment
Part A: Your information
1 |
Marital status |
|
single |
married |
separated |
|
|
|
|
|
|
If married, complete your spouse’s information in Part B. |
|
|
|
|
|
||||
2 |
Your name ___________________________________________ 11 |
Filing status |
single |
married filing jointly |
||||||
3 Street address ________________________________________ |
|
|
head of household |
married filing separately |
||||||
|
____________________________________________________ 12 |
Average monthly |
||||||||
|
City |
|
|
State |
ZIP |
13 |
Amounts withheld from your paycheck (e.g., savings, bonds, |
|||
|
|
|
|
|
|
|||||
4 |
Home phone (____)____________________________________ |
|
deferred amounts, car payments, etc.) $______________________ |
|||||||
5 |
Social Security number |
___ ___ ___- ___ ___- ___ ___ ___ ___ |
|
______________________________________________________ |
||||||
6 |
Unemployed |
yes |
no If “yes,” how long. _______________ 14 |
Dates paid _____________________________________________ |
||||||
7 |
Current or former employer’s name ________________________ 15 |
Length of employment ____________________________________ |
||||||||
8 |
Address _____________________________________________ 16 |
Date of birth |
___ ___/___ ___/___ ___ ___ ___ |
|
||||||
|
____________________________________________________ 17 |
Name and address of next of kin (other than spouse) |
|
|||||||
|
City |
|
|
State |
ZIP |
|
Name ________________________________________________ |
|||
|
|
|
|
|
|
|
||||
9 |
Work phone (_____)____________________________________ |
|
Street address _________________________________________ |
|||||||
10 |
Occupation___________________________________________ |
|
______________________________________________________ |
|||||||
|
|
|
|
|
|
|
City |
|
State |
ZIP |
Part B: Your spouse’s information
18 |
Spouse’s name _______________________________________ 25 |
Work phone(_____)______________________________________ |
||||
19 |
Address (if different)____________________________________ 26 |
Occupation ____________________________________________ |
||||
|
____________________________________________________ 27 |
Average monthly |
||||
|
City |
|
State |
ZIP |
28 |
Amounts withheld from your paycheck (e.g., savings, bonds, |
|
|
|
|
|
||
20 |
Home phone (if different)(_____)__________________________ |
|
deferred amounts, car payments, etc.) $______________________ |
|||
21 |
Social Security number |
___ ___ |
|
______________________________________________________ |
||
22 |
Unemployed |
yes |
no If “yes,” how long._______________ 29 |
Dates paid _____________________________________________ |
||
23 |
Current or former employer’s name ________________________ 30 |
Length of employment ____________________________________ |
||||
24 |
Address _____________________________________________ 31 |
Date of birth ___ ___/___ ___/___ ___ ___ ___ |
||||
|
____________________________________________________ |
|
|
|||
|
City |
|
State |
ZIP |
|
|
Section 2: Complete the following financial information
Note: Attach additional sheets in the same format for any of the following parts if necessary.
Part A: Your bank accounts (include savings and loans, credit unions, IRA and retirement plans, and certificates of deposit)
|
A |
B |
C |
D |
E |
|
|
|
Type of |
Account |
|
|
Name of institution |
Address |
account |
number |
Balance |
32 |
______________________ |
_______________________________________ |
___________ |
___________ |
____________ |
33______________________ |
_______________________________________ |
___________ |
___________ |
____________ |
|
34 |
______________________ |
_______________________________________ |
___________ |
___________ |
____________ |
35 |
______________________ |
_______________________________________ |
___________ |
___________ |
____________ |
36 |
______________________ |
_______________________________________ |
___________ |
___________ |
____________ |
37______________________ |
_______________________________________ |
___________ |
___________ |
____________ |
|
38 |
Add Lines 32 through 37, Column E, and write the total here and on Part G, Line 56, Column B. |
38 |
____________ |
||
Page 1 of 4 |
Part B: Your charge cards or credit lines from your banks, credit unions, and savings and loans
|
A |
B |
C |
|
Type of account |
|
Current |
|
or card |
Name and address of financial institution |
balance |
39 |
_________________ |
_______________________________________________________________________ |
___________ |
40 |
_________________ |
_______________________________________________________________________ |
___________ |
41 |
_________________ |
_______________________________________________________________________ |
___________ |
42 |
_________________ |
_______________________________________________________________________ |
___________ |
43 |
_________________ |
_______________________________________________________________________ |
___________ |
44 |
Add Lines 39 through 43, Column C, and write the total here and on Part G, Line 57, Column C. |
44 ___________ |
|
Part C: Real property you own
|
A |
B |
C |
D |
|
Brief description |
How property |
|
|
|
of property |
is titled |
Physical address |
County |
45 |
_____________________________ |
__________________ |
_______________________________________ |
___________ |
46 |
_____________________________ |
__________________ |
_______________________________________ |
___________ |
47 |
_____________________________ |
__________________ |
_______________________________________ |
___________ |
Part D: Your life and health insurance policies
|
A |
B |
C |
D |
E |
|
|
Policy |
|
Face |
Available |
|
Insurance company |
number |
Type |
amount |
loan value |
48 |
__________________________________________________ |
___________ |
___________ |
___________ |
___________ |
49 |
__________________________________________________ |
___________ |
___________ |
___________ |
___________ |
50 |
Add Lines 48 and 49, Column E, and write the total here and on Part G, Line 60, Column B. |
|
50 ___________ |
||
Part E: Your securities (e.g., stocks, bonds, annuities, mutual funds, money market funds, government securities, notes, personal, etc.)
|
A |
B |
C |
D |
E |
|
Type |
|
|
Quantity or |
|
|
of security |
Location |
Owner of record |
denomination |
Present value |
51 |
_________________ |
______________________________ |
_________________________ |
___________ |
___________ |
52 |
_________________ |
______________________________ |
_________________________ |
___________ |
___________ |
53 |
Add Lines 51 and 52, Column E, and write the total here and on Part G, Line 61, Column B. |
|
53 ___________ |
||
Part F: Miscellaneous information
54a Are foreclosure, bankruptcy, receivership, or assignment for benefit of creditors proceedings pending? b What is the bankruptcy number? ______________________
Yes
No
c What date was the bankruptcy filed? ___ ___/___ ___/___ ___ ___ ___ |
If closed, what was the date? ___ ___/___ ___/___ ___ ___ ___ |
||||
Month |
Day |
Year |
Month |
Day |
Year |
Page 2 of 4 |

Part G: Analyze your assets and liabilities
Note: Write amounts in all unshaded areas that apply
|
A |
B |
|
|
Fair market |
|
Description |
value |
55 |
Cash |
___________ |
56 |
Total bank accounts |
|
|
from Section 2, Part A, |
|
|
Line 38 |
___________ |
57Total charge cards balance from Section 2, Part B,
Line 44 |
___________ |
58Vehicles (model, year)
a ___________________ |
___________ |
|
b ___________________ |
___________ |
|
c ___________________ |
___________ |
|
59 |
Real property listed |
|
|
in Section 2, |
|
|
Part C, (Line 45) |
___________ |
|
(Line 46) |
___________ |
|
(Line 47) |
___________ |
60 |
Total cash or loan value |
|
|
of insurance from |
|
|
Section 2, Part D, |
|
|
Line 50 |
___________ |
61 |
Total securities from |
|
|
Section 2, Part E, |
|
|
Line 53 |
___________ |
62 |
Other assets (specify) |
|
C
Liabilities
balance due
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
D
Equity
(Column B minus
Column C)
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
E
Monthly payment amount
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
F
Pledgee or obligee
___________________
___________________
___________________
___________________
___________________
___________________
___________________
___________________
___________________
___________________
___________________
G
Date of
final
payment
____________
____________
____________
____________
____________
____________
____________
____________
____________
____________
____________
a___________________
b___________________
c___________________
63 Other liabilities not covered above (e.g., judgments, charities, tuition)
a___________________
b___________________
c___________________
64 Federal taxes owed
65 State taxes owed a Illinois individual
income tax
b Illinois business income tax
c Other state taxes
66Total
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________
___________________
___________________
___________________
___________________
___________________
___________________
___________________
___________________
___________________
___________________
___________________
____________
____________
____________
____________
____________
____________
____________
____________
____________
____________
____________
Page 3 of 4 |
Part H: Analyze your monthly income and expenses
Income
|
A |
B |
C |
|
Source |
Gross |
Net |
67 |
Your wages or salary |
___________________ |
___________________ |
68 |
Your spouse’s |
|
|
|
wages or salary |
___________________ |
___________________ |
69 |
Interest or dividends |
___________________ |
___________________ |
70 |
Business income |
___________________ |
___________________ |
71 |
Rental income |
___________________ |
___________________ |
72 |
Your pension |
___________________ |
___________________ |
73 |
Your spouse’s pension |
___________________ |
___________________ |
74 |
Child support |
___________________ |
___________________ |
75 |
Alimony |
___________________ |
___________________ |
76Other (specify)
________________ ___________________ ___________________
________________ ___________________ ___________________
________________ ___________________ ___________________
________________ ___________________ ___________________
________________ ___________________ ___________________
________________ ___________________ ___________________
________________ ___________________ ___________________
________________ |
___________________ |
___________________ |
________________ |
___________________ |
___________________ |
________________ |
___________________ |
___________________ |
________________ |
___________________ |
___________________ |
________________ |
___________________ |
___________________ |
77 Add Lines 67 through 76, Column C. |
|
|
This amount is your total net income. |
____________________ |
|
Necessary monthly living expenses
A |
B |
Expense |
Amount |
78Rent (not included
|
in Part G, Line 59) |
___________________ |
||
79 |
Groceries |
|
|
|
|
(number of people____) |
___________________ |
||
80 |
Installment pmts. from |
|
||
|
Part G, Line 66, Col. E |
___________________ |
||
81 |
Utilities |
a |
gas |
___________________ |
|
|
b |
water |
___________________ |
|
|
c |
electric |
___________________ |
|
|
d |
telephone |
___________________ |
82 |
Transportation |
___________________ |
||
83 |
Insurance |
a |
life |
___________________ |
|
(monthly |
b |
health |
___________________ |
|
premiums) c |
home |
___________________ |
|
|
|
d |
car |
___________________ |
84Medical (not covered
|
in Line 83b above) |
___________________ |
85 |
Estimated tax payments |
___________________ |
86 |
___________________ |
87Other (specify)
__________________ ___________________
__________________ ___________________
__________________ ___________________
88Add Lines 78 through 87. This amount is your
total expenses. |
___________________ |
89 Subtract Line 88 from Line 77. This amount is your net income after expenses. |
89 ___________________ |
Part I: Complete any additional asset or income information
90Write any additional information you have about your assets or income that was not included in any of the preceding parts. Be sure to include a statement regarding the prospect of any increase in the value of your assets or your present income.
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Section 3: Sign below
Under penalties of perjury, I state that I have examined this statement of assets, liabilities, and other information and, to the best of my knowledge, it is true, correct, and complete.
______________________________________________/___/_____ ______________________________________________/___/_____
Petitioner’s signature (not representative) |
Date |
Spouse’s signature |
Date |
Page 4 of 4
This form is authorized as outlined by the Illinois Income Tax Act. Disclosure of this information is REQUIRED. Failure to provide information |
|
|
could result in this form not being processed. This form has been approved by the Forms Management Center. |
||
|
|
|
|
|
|
Document Breakdown
| Fact Name | Description |
|---|---|
| Form Purpose | The Illinois BOA-4 form is used to collect financial information from individuals for tax assessment purposes. |
| Governing Law | This form is authorized under the Illinois Income Tax Act. |
| Marital Status Options | Individuals must indicate their marital status, selecting from options such as single, married, separated, or head of household. |
| Employment Information | Section 1 of the form requires details about the individual's employment, including current or former employer's name and length of employment. |
| Financial Disclosure | Part 2 requires individuals to disclose bank accounts, charge cards, real property, and various insurance policies. |
| Next of Kin | Individuals must provide the name and address of a next of kin, other than a spouse, for contact purposes. |
| Income and Expenses | Part H analyzes monthly income and expenses, requiring individuals to detail sources of income and necessary living expenses. |
| Signature Requirement | The form must be signed by the petitioner and, if applicable, by the spouse, under penalties of perjury. |
| Penalties for Non-Disclosure | Failure to provide required information may result in the form not being processed by the Illinois Department of Revenue. |
| Form Version | The current version of the BOA-4 form is R-4/01, as indicated on the document. |
Create More PDFs
Charitable Trust Bureau - By providing net asset details, the form gives insight into the organization’s financial stability and growth.
The Florida Small Estate Affidavit form is a crucial document that simplifies the process of handling smaller estates. For those seeking to avoid the complexities of formal probate, an understanding of the clear path to small estate affidavit usage can be highly beneficial.
Illinois Iema 243 - It is a critical component of the state's laser safety framework, underlining the importance of regulatory compliance.