Fill a Valid Illinois First Report 45 Form
The Illinois First Report 45 form is a crucial document that employers must complete when a work-related injury occurs. Designed to capture essential information, this form helps ensure that both employees and employers navigate the complexities of workers' compensation effectively. Key details required include the employer's information, such as the Federal Employer Identification Number (FEIN), business name, and mailing address. It also asks for specifics about the injured employee, including their name, birthdate, and job title. Understanding whether the incident resulted in lost workdays is vital, as this can influence the reporting process. The form delves into the circumstances surrounding the accident, requesting descriptions of what the employee was doing at the time, how the injury occurred, and the nature of the injury itself. Additional inquiries cover medical treatment received, including whether the employee was treated in an emergency room or hospitalized. By gathering this information, the form serves not only as a report to the Illinois Workers' Compensation Commission but also as a means for employers to maintain compliance with legal requirements. Remember, filing this form is a step toward protecting both the rights of the injured employee and the interests of the employer.
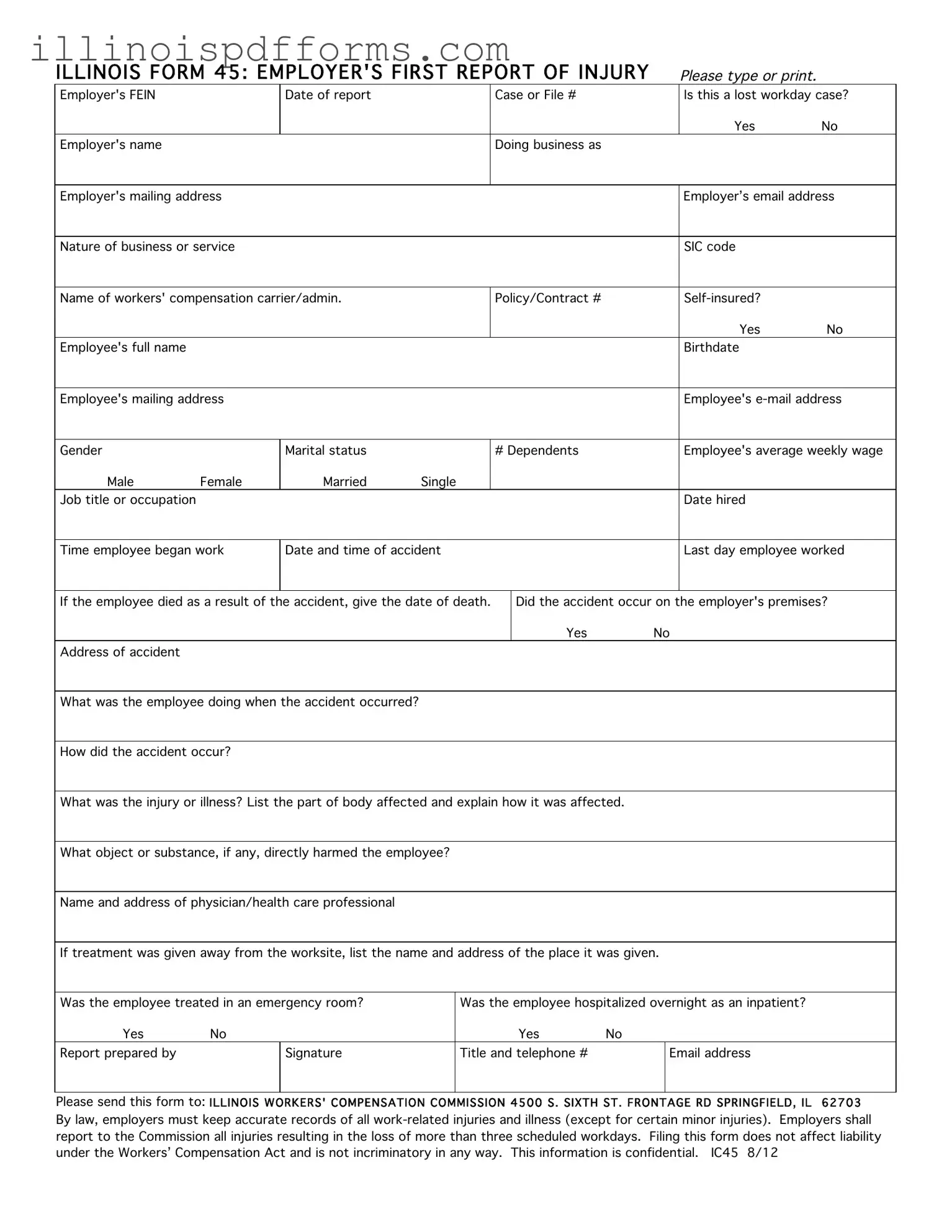
Example - Illinois First Report 45 Form

ILLINOIS FORM 45: EMPLOYER'S FIRST REPORT OF INJURY |
|
|
Please type or print. |
|
|||||||||
Employer's FEIN |
|
Date of report |
|
|
|
|
Case or File # |
|
|
|
Is this a lost workday case? |
||
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
Employer's name |
|
|
|
|
|
|
Doing business as |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Employer's mailing address |
|
|
|
|
|
|
|
|
|
|
Employer’s email address |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nature of business or service |
|
|
|
|
|
|
|
|
|
|
SIC code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Name of workers' compensation carrier/admin. |
|
|
|
|
Policy/Contract # |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
Employee's full name |
|
|
|
|
|
|
|
|
|
|
|
Birthdate |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Employee's mailing address |
|
|
|
|
|
|
|
|
|
|
Employee's |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Gender |
|
Marital status |
|
|
|
|
# Dependents |
|
|
|
Employee's average weekly wage |
||
Male |
Female |
Married |
Single |
|
|
|
|
|
|
|
|
|
|
Job title or occupation |
|
|
|
|
|
|
|
|
|
|
|
Date hired |
|
|
|
|
|
|
|
|
|
|
|
|
|||
Time employee began work |
Date and time of accident |
|
|
|
|
|
|
|
Last day employee worked |
||||
|
|
|
|
|
|
|
|||||||
If the employee died as a result of the accident, give the date of death. |
|
Did the accident occur on the employer's premises? |
|||||||||||
|
|
|
|
|
|
|
|
Yes |
|
No |
|
||
Address of accident |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
What was the employee doing when the accident occurred? |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
How did the accident occur? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
What was the injury or illness? List the part of body affected and explain how it was affected. |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|||
What object or substance, if any, directly harmed the employee? |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||
Name and address of physician/health care professional |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||||||||||
If treatment was given away from the worksite, list the name and address of the place it was given. |
|
||||||||||||
|
|
|
|
|
|
||||||||
Was the employee treated in an emergency room? |
|
|
Was the employee hospitalized overnight as an inpatient? |
|
|||||||||
Yes |
No |
|
|
|
|
|
|
Yes |
No |
|
|
|
|
Report prepared by |
|
Signature |
|
|
Title and telephone # |
|
|
Email address |
|
||||
|
|
|
|
|
|||||||||
Please send this form to: ILLINOIS WORKERS' COMPENSATION COMMISSION 4500 S. SIXTH ST. FRONTAGE RD SPRINGFIELD, IL |
62703 |
||||||||||||
By law, employers must keep accurate records of all
Document Breakdown
| Fact Name | Description |
|---|---|
| Purpose | The Illinois First Report 45 form is used by employers to report work-related injuries or illnesses to the Illinois Workers' Compensation Commission. |
| Governing Law | This form is governed by the Illinois Workers' Compensation Act, which mandates reporting of certain injuries. |
| Lost Workday Cases | Employers must indicate if the reported case involves lost workdays, which triggers specific reporting requirements. |
| Confidentiality | The information provided in the form is confidential and is protected under Illinois law. |
| Submission Requirements | Employers are required to submit this form to the Illinois Workers' Compensation Commission within a specified timeframe following an incident. |
| Record-Keeping Obligation | Employers must maintain accurate records of all work-related injuries and illnesses, as mandated by law. |
| Non-Incriminatory | Filing the First Report 45 form does not affect the employer's liability under the Workers' Compensation Act and is not considered an admission of guilt. |
Create More PDFs
Illinois State Id Card - Enhanced security features on Illinois’s new Driver’s Licenses are set to significantly cut down on identity theft and license fraud.
Foid Card Application Chicago - The application requires personal information, including height, weight, date of birth, and hair color, to be completed by the applicant.