Fill a Valid Illinois Hfs 2243 Form
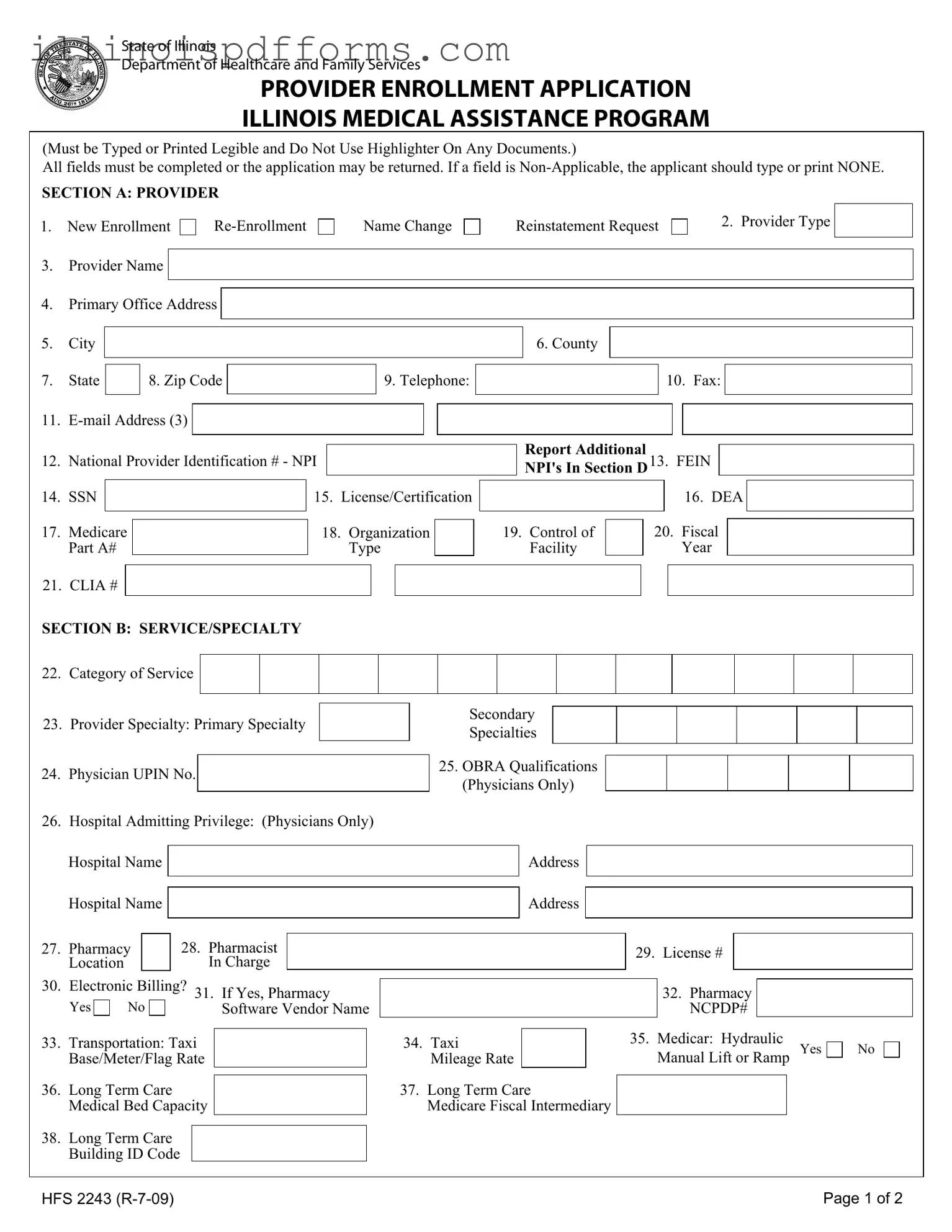
The Illinois HFS 2243 form is a crucial document for healthcare providers seeking enrollment in the Illinois Medical Assistance Program. This application requires careful attention to detail, as all fields must be completed accurately to avoid delays or rejections. The form covers various aspects of provider information, including the type of enrollment—whether it is a new enrollment, re-enrollment, name change, or reinstatement request. Essential details such as the provider's name, address, National Provider Identification (NPI) number, and contact information must be provided. Additionally, the form includes sections that address service categories and specialties, allowing providers to specify their primary and secondary specialties. For physicians, specific qualifications and hospital admitting privileges are also required. The form further necessitates the disclosure of any prior participation in the program, and it includes a certification section where the provider affirms the accuracy of the information submitted. Compliance with federal and state laws is emphasized, ensuring that all applicants are aware of the legal implications of providing false information. By completing the HFS 2243 form, healthcare providers can take a significant step toward participating in a program that supports access to medical services for those in need.
Example - Illinois Hfs 2243 Form
State of Illinois
Department of Healthcare and Family Services
PROVIDER ENROLLMENT APPLICATION
ILLINOIS MEDICAL ASSISTANCE PROGRAM
(Must be Typed or Printed Legible and Do Not Use Highlighter On Any Documents.)
All fields must be completed or the application may be returned. If a field is
SECTION A: PROVIDER
1.New Enrollment
3.Provider Name
Name Change
Reinstatement Request
2. Provider Type
4.Primary Office Address
5.City
6. County
7.State
8. Zip Code
9. Telephone:
10. Fax:
11. |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
12. |
National Provider Identification # - NPI |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
14. |
SSN |
|
|
|
15. |
License/Certification |
|||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
||||
17. |
Medicare |
|
|
18. |
Organization |
|
|||
|
Part A# |
|
|
|
|
Type |
|
||
Report Additional
NPI's In Section D13. FEIN
|
|
|
16. DEA |
|
|
|
|
|
|
|
|
19. Control of |
|
20. Fiscal |
|
|
|
|
|
|
|||
Facility |
|
|
Year |
|
|
21. CLIA #
SECTION B: SERVICE/SPECIALTY
22.Category of Service
23.Provider Specialty: Primary Specialty
24.Physician UPIN No.
Secondary
Specialties
25.OBRA Qualifications (Physicians Only)
26. Hospital Admitting Privilege: (Physicians Only)
|
Hospital Name |
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hospital Name |
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
28. Pharmacist |
|
|
|
|
|
|
|
|
|
|
|
|||
27. |
Pharmacy |
|
|
|
|
|
|
|
|
29. |
License # |
|
|
|
|||
|
Location |
|
|
|
In Charge |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
30. |
Electronic Billing? 31. If Yes, Pharmacy |
|
|
|
|
|
32. Pharmacy |
|
|
||||||||
|
|
|
|
|
|
|
|||||||||||
|
Yes |
No |
|
Software Vendor Name |
|
|
|
|
|
NCPDP# |
|
|
|||||
33. |
Transportation: Taxi |
|
|
|
34. Taxi |
|
|
|
35. |
Medicar: Hydraulic |
|||||||
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
Manual Lift or Ramp Yes |
|||||||||||
|
Base/Meter/Flag Rate |
|
|
Mileage Rate |
|
|
|
|
|||||||||
36. |
Long Term Care |
|
|
|
|
37. Long Term Care |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||||||||
|
Medical Bed Capacity |
|
|
Medicare Fiscal Intermediary |
|
|
|
|
|
|
|||||||
38.Long Term Care Building ID Code
No
HFS 2243 |
Page 1 of 2 |
SECTION C: FORMER PARTICIPATION
39. Change of Ownership |
Yes |
40. Former Provider Number
No
Effective Date
Former Provider Name
SECTION D: ADDITIONAL NPI - National Provider Identification #
41. NPI
NPI
SECTION E: PAYEE INFORMATION
NPI
NPI
NPI
NPI
42. Name
44.DBA
45.Street Address
46.City
50.SSN/FEIN
52.Medicare Part B#
43. Telephone:
47. State |
|
|
|
48. Zip Code |
|
|
|
|
49. TIN Type Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
51. Billing Provider/Pay To NPI # |
|
|
|
|
|||
|
53. PIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
54. DMERC# |
|
|
|
|||
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
Name
DBA
Street Address
Telephone:
City |
|
|
|
|
State |
|
|
Zip Code |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
SSN/FEIN |
|
|
|
|
|
|
Billing Provider/Pay To NPI # |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|||||
Medicare Part B# |
|
PIN |
|
|
|
|
|
DMERC# |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
||
SECTION F: CERTIFICATION/SIGNATURE |
|
|
|
|
|
|
|
|
|
|
|||
TIN Type Code
I understand that knowingly falsifying or willfully withholding information may be cause for the denial or termination of participation in the Medical Assistance Program and such conduct may be prosecuted under applicable Federal and State laws..
Under penalties of perjury, I hereby certify that all of the information provided in this application process is true, correct and complete and that the enrolling provider is in compliance with all applicable federal and state laws and regulations. I further certify that neither I, nor any of the following provider's employees, partners, officers, or shareholders owning at least five percent (5%) of said provider are currently barred, suspended, terminated, voluntarily withdrawn as part of a settlement agreement, or otherwise excluded from participation in the Medicaid or Medicare programs, nor are any of the above currently under sanction for, or serving a sentence for conviction of any Medicaid or Medicare program violations. I further certify that none of the above are currently sanctioned by any federal agency for any reason. I authorize the Department of Healthcare and Family Services, to verify the information provided on this application with other state and federal agencies. I further certify that I will review and comply with the Department's policies, rules and regulations including but not limited to those found at the following websites:
Illinois HFS website address: http://www.hfs.illinois.gov/
Illinois HFS Handbook updates are available: http://www.hfs.illinois.gov/handbooks
Illinois HFS Laws and Rule Regulations: http://www.hfs.illinois.gov/lawsrules/index.html
Signature:
Printed name of person signing above
Check this box if you want a provider handbook mailed
Date
HFS 2243 |
Page 2 of 2 |
Document Breakdown
| Fact Name | Details |
|---|---|
| Form Purpose | The HFS 2243 form is used for provider enrollment in the Illinois Medical Assistance Program. |
| Eligibility | Providers must complete all fields; incomplete applications may be returned. |
| Non-Applicable Fields | If a field does not apply, the applicant should indicate "NONE" in that section. |
| Sections | The form consists of multiple sections, including Provider Information, Service/Specialty, and Certification/Signature. |
| Provider Types | Options include new enrollment, re-enrollment, name change, and reinstatement requests. |
| Governing Laws | This form is governed by the Illinois Compiled Statutes, specifically under healthcare regulations. |
| Electronic Billing | Providers can indicate if they will use electronic billing, which is an option on the form. |
| Certification Requirement | Applicants must certify that all information is true and that they comply with federal and state laws. |
| Verification Authorization | By signing, applicants authorize the Department of Healthcare and Family Services to verify provided information. |
Create More PDFs
What Does Rule to Vacate Mean - For tenants, receiving this form signifies the need to commence the search for new accommodation promptly.
To facilitate the divorce process, it is crucial to utilize the California Divorce Settlement Agreement form, which clearly specifies the distribution of assets, debts, and custody arrangements. For those looking to streamline this essential legal procedure, you can find helpful resources at California Templates.
Child Support Estimator Illinois - By addressing prior support orders actually paid, the form takes into account the non-custodial parent's existing financial responsibilities.
Il-1040 Form 2023 - This form helps Illinois taxpayers report credits like the Illinois Property Tax Credit and K-12 Education Expense Credit.