Fill a Valid Illinois Income Verification Form
Navigating the world of income verification can feel overwhelming, especially for those seeking assistance through programs like the Child Care Assistance Program (CCAP) in Illinois. The Illinois Income Verification form plays a crucial role in this process. It serves as a bridge between employees and their employers, ensuring that accurate income information is submitted for eligibility assessments. This form requires the employee to provide their personal details, including their name and case number, and to authorize their employer to release necessary income information. Employers, in turn, are tasked with filling out key sections about the business, the employee's work schedule, and their compensation structure. This includes details such as the employee's gross pay, hours worked per week, and payment frequency. It's important to note that this form is not just a one-time requirement; it is designed for initial eligibility and may need to be updated during the next redetermination process. By understanding the purpose and requirements of the Illinois Income Verification form, individuals can better prepare for the verification process and ensure they receive the support they need.
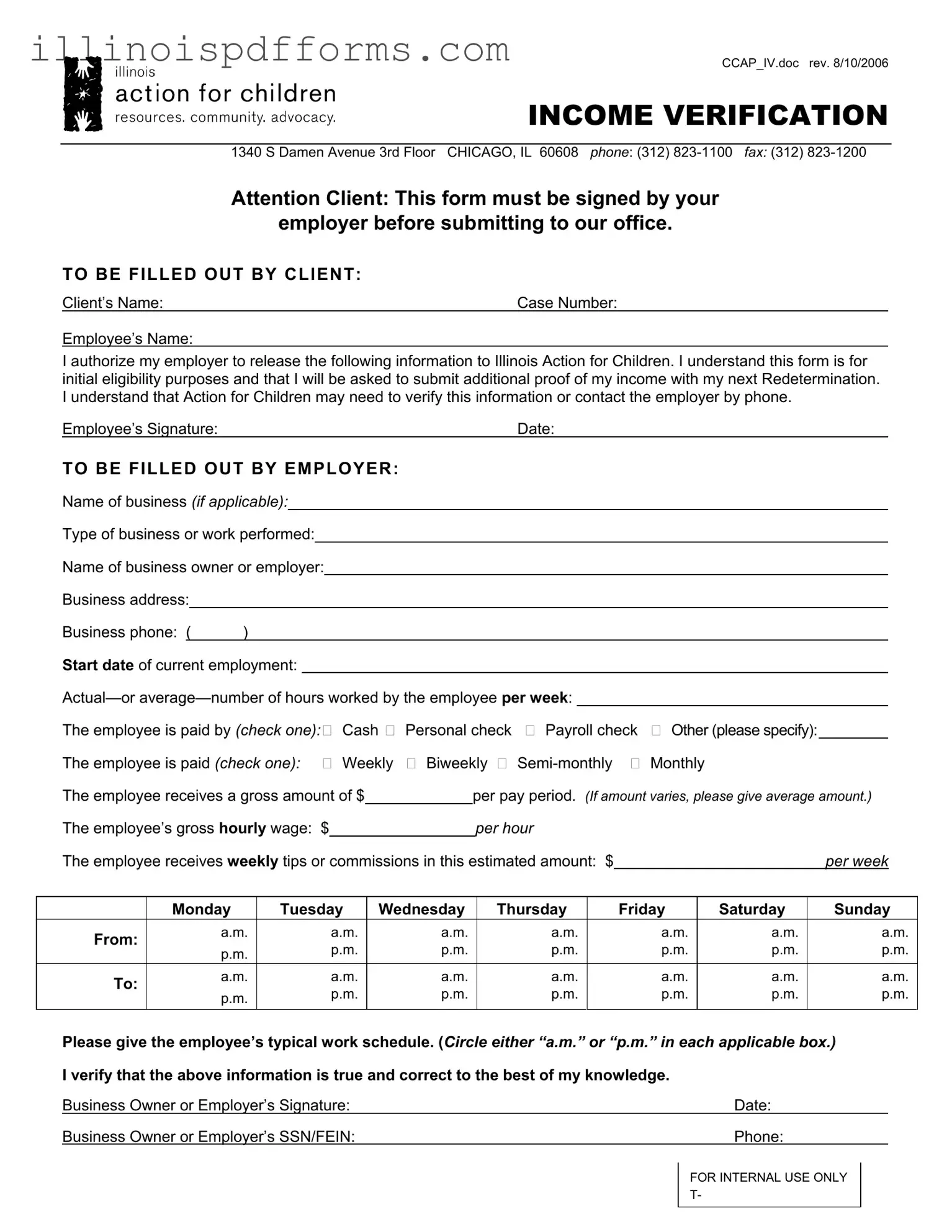
Example - Illinois Income Verification Form
CCAP_IV.doc rev. 8/10/2006
INCOME VERIFICATION
1340 S Damen Avenue 3rd Floor CHICAGO, IL 60608 phone: (312)
Attention Client: This form must be signed by your
employer before submitting to our office.
TO BE FILLED OUT BY CLIENT:
Client’s Name: |
Case Number: |
Employee’s Name:
I authorize my employer to release the following information to Illinois Action for Children. I understand this form is for initial eligibility purposes and that I will be asked to submit additional proof of my income with my next Redetermination. I understand that Action for Children may need to verify this information or contact the employer by phone.
Employee’s Signature: |
Date: |
TO BE FILLED OUT BY EMPLOYER:
Name of business (if applicable):
Type of business or work performed:
Name of business owner or employer:
Business address:
|
|
Business phone: ( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Start date of current employment: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
The employee is paid by (check one): Cash Personal check Payroll check Other (please specify): |
|
|
|
|
|||||||||||||||||
|
|
The employee is paid (check one): |
Weekly Biweekly |
Monthly |
|
|
|
|
|||||||||||||||
|
|
The employee receives a gross amount of $ |
|
|
per pay period. (If amount varies, please give average amount.) |
||||||||||||||||||
|
|
The employee’s gross hourly wage: $ |
|
|
|
|
per hour |
|
|
|
|
|
|
|
|
|
|||||||
|
|
The employee receives weekly tips or commissions in this estimated amount: $ |
|
|
|
|
|
per week |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
Monday |
|
Tuesday |
|
Wednesday |
|
Thursday |
|
Friday |
|
Saturday |
|
Sunday |
|
|||||||
|
|
From: |
|
a.m. |
|
|
a.m. |
|
a.m. |
|
a.m. |
|
a.m. |
|
a.m. |
|
|
a.m. |
|
||||
|
|
|
p.m. |
|
|
p.m. |
|
p.m. |
|
p.m. |
|
p.m. |
|
p.m. |
|
|
p.m. |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
To: |
|
a.m. |
|
|
a.m. |
|
a.m. |
|
a.m. |
|
a.m. |
|
a.m. |
|
|
a.m. |
|
||||
|
|
|
p.m. |
|
|
p.m. |
|
p.m. |
|
p.m. |
|
p.m. |
|
p.m. |
|
|
p.m. |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Please give the employee’s typical work schedule. (Circle either “a.m.” or “p.m.” in each applicable box.) |
|||||||||||||||||||||
|
|
I verify that the above information is true and correct to the best of my knowledge. |
|
|
|
|
|
|
|
||||||||||||||
|
|
Business Owner or Employer’s Signature: |
|
|
|
|
|
|
|
|
|
Date: |
|
|
|
|
|||||||
|
|
Business Owner or Employer’s SSN/FEIN: |
|
|
|
|
|
|
|
|
|
Phone: |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FOR INTERNAL USE ONLY |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
T- |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Document Breakdown
| Fact Name | Description |
|---|---|
| Purpose | The Illinois Income Verification form is used to verify income for eligibility purposes, particularly for programs administered by Illinois Action for Children. |
| Employer Signature Required | Before submission, the form must be signed by the employer to validate the information provided by the employee. |
| Client Information | Clients must fill out their name, case number, and employee’s name as part of the form. |
| Authorization | Clients authorize their employers to release income information to Illinois Action for Children, which is crucial for processing their application. |
| Verification Process | Illinois Action for Children may contact the employer by phone to verify the income information provided in the form. |
| Frequency of Payment | The form requires employers to indicate how often the employee is paid, such as weekly, biweekly, semi-monthly, or monthly. |
| Governing Law | This form is governed by the Illinois Administrative Code, specifically related to eligibility determinations for state assistance programs. |
| Work Schedule | Employers must provide the employee’s typical work schedule, detailing hours worked each day of the week. |
| Internal Use | The form contains a section marked for internal use only, indicating that additional processing may occur after submission. |
Create More PDFs
How to Change President of Corporation Illinois - Maintain legal compliance for your Illinois LLC by updating your registered agent and office address with this document.
When engaging in real estate transactions, understanding the specifics of a Real Estate Purchase Agreement is crucial. This document not only facilitates the sale but also clarifies the responsibilities of both parties, ensuring a smoother process during property exchanges in Florida.
Charitable Trust Bureau - Detailed reporting on fundraising expenses versus amounts raised assesses the efficiency and effectiveness of those efforts.
Can I Send My Child to a Different School District - A mechanism for Illinois schools to assess and accept transfer students based on their disciplinary history and health records.