Fill a Valid Illinois Placard Form
The Illinois Placard form serves as a crucial document for individuals with disabilities seeking parking accommodations. This form is designed for both new applicants and those looking to renew their existing placards. It is important to note that if a placard has been lost, stolen, or damaged, a replacement form must be utilized instead. The certification process requires a physician's signature, which validates the applicant's disability status and eligibility for either a temporary or permanent parking placard. For temporary placards, the certification is valid for three months, while permanent placards are valid for six months. The form necessitates thorough completion of all sections, with specific requirements for minors, who must have their parent or guardian fill out additional parts. Medical professionals must also provide detailed information about the applicant's disability, including the nature and duration of the condition. Furthermore, individuals applying for meter-exempt parking must meet additional criteria outlined in the form. Misuse of the placard can lead to serious consequences, including fines and license revocation. The application process can be initiated at any Secretary of State facility or via mail, depending on the type of placard being applied for. Understanding the intricacies of this form is essential for ensuring that individuals with disabilities receive the accommodations they require to navigate their communities effectively.
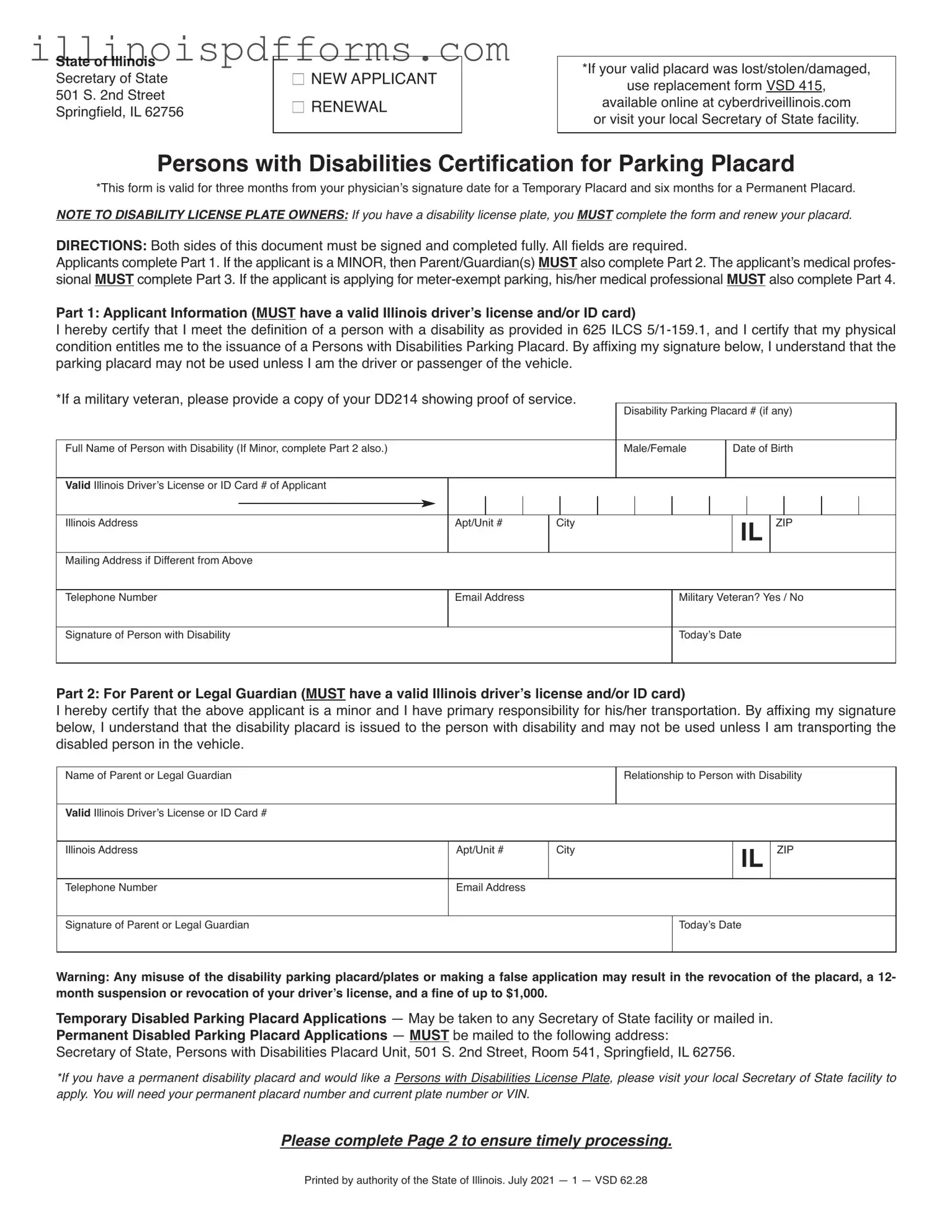
Example - Illinois Placard Form
State of Illinois Secretary of State 501 S. 2nd Street Springfield, IL 62756
NNEW APPLICANT
NRENEWAL
*If your valid placard was lost/stolen/damaged,
use replacement form VSD 415,
available online at cyberdriveillinois.com or visit your local Secretary of State facility.
Persons with Disabilities Certification for Parking Placard
*This form is valid for three months from your physician’s signature date for a Temporary Placard and six months for a Permanent Placard.
NOTE TO DISABILITY LICENSE PLATE OWNERS: If you have a disability license plate, you MUST complete the form and renew your placard.
DIRECTIONS: Both sides of this document must be signed and completed fully. All fields are required.
Applicants complete Part 1. If the applicant is a MINOR, then Parent/Guardian(s) MUST also complete Part 2. The applicant’s medical profes- sional MUST complete Part 3. If the applicant is applying for
Part 1: Applicant Information (MUST have a valid Illinois driver’s license and/or ID card)
I hereby certify that I meet the definition of a person with a disability as provided in 625 ILCS
*If a military veteran, please provide a copy of your DD214 showing proof of service.
|
|
|
|
|
|
|
|
Disability Parking Placard # (if any) |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Full Name of Person with Disability (If Minor, complete Part 2 also.) |
|
|
|
|
|
Male/Female |
|
Date of Birth |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Valid Illinois Driver’s License or ID Card # of Applicant |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Illinois Address |
Apt/Unit # |
City |
|
|
|
|
|
IL |
ZIP |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address if Different from Above |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone Number |
Email Address |
|
|
|
|
Military Veteran? Yes / No |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of Person with Disability |
|
|
|
|
|
|
|
Today’s Date |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Part 2: For Parent or Legal Guardian (MUST have a valid Illinois driver’s license and/or ID card)
I hereby certify that the above applicant is a minor and I have primary responsibility for his/her transportation. By affixing my signature below, I understand that the disability placard is issued to the person with disability and may not be used unless I am transporting the disabled person in the vehicle.
Name of Parent or Legal Guardian |
|
|
Relationship to Person with Disability |
|||
|
|
|
|
|
|
|
Valid Illinois Driver’s License or ID Card # |
|
|
|
|
|
|
|
|
|
|
|
|
|
Illinois Address |
Apt/Unit # |
City |
|
|
IL |
ZIP |
|
|
|
|
|
|
|
Telephone Number |
Email Address |
|
|
|
|
|
|
|
|
|
|
|
|
Signature of Parent or Legal Guardian |
|
|
|
Today’s Date |
||
|
|
|
|
|
|
|
Warning: Any misuse of the disability parking placard/plates or making a false application may result in the revocation of the placard, a 12- month suspension or revocation of your driver’s license, and a fine of up to $1,000.
Temporary Disabled Parking Placard Applications — May be taken to any Secretary of State facility or mailed in. Permanent Disabled Parking Placard Applications — MUST be mailed to the following address:
Secretary of State, Persons with Disabilities Placard Unit, 501 S. 2nd Street, Room 541, Springfield, IL 62756.
*If you have a permanent disability placard and would like a Persons with Disabilities License Plate, please visit your local Secretary of State facility to apply. You will need your permanent placard number and current plate number or VIN.
Please complete Page 2 to ensure timely processing.
Printed by authority of the State of Illinois. July 2021 — 1 — VSD 62.28

Part 3: Medical Eligibility Standards and Medical Professional Certification
As the medical professional(s) executing this document and verifying the nature of the applicant’s disability, I understand that making a false representation of a person’s disability for the purposes of obtaining any type of disabled parking placard may result in suspension or revocation of my license and a fine of up to $1,000. As a licensed physician, advanced practiced nurse, optometrist, chiropractor or physician’s assistant, I certify the applicant has a condition that constitutes him/her as a person with disabilities.
Length of Disability: (Check one)
NTemporary Disability; the duration of this disability is ________________________(maximum 6 months)
NPermanent Disability
N
Check all that apply: (MUST check at least one):
NIs restricted by a lung disease to such a degree that the person’s forced (respiratory) expiratory volume (FEV) for 1 second, when measured by spirometry, is less than 1 liter.
NUses a portable oxygen device.
NHas Class III or Class IV cardiac condition according to the standards set by the American Heart Association.
NCannot walk without the use of or assistance from a wheelchair, a walker, a crutch, a brace, a prosthetic device, or another person.
NIs severely limited in the ability to walk due to an arthritic, neurological, oncological, or orthopedic condition.
NCannot walk 200 feet without stopping to rest because of one of the above five conditions.
Check all that apply: (MUST check at least one diagnosis): |
|
|
N Amputation of extremity(s) _________________________ |
N Arthritis of the ______________________________________ |
|
N Spina Bifida |
N Osteoarthritis of the |
_________________________________ |
N Multiple Sclerosis |
N Chronic Pain due to |
_________________________________ |
N Quadriplegia/Paraplegia |
N Legally Blind with limited mobility |
|
NCerebral Palsy
NOther Diagnosis: _________________________________________________________________________________________
If none of the above conditions apply, list the medical condition that impacts the person’s mobility.
Medical Professional’s Printed Name |
Specialty |
|
|
|
|
Office Address |
City, State, ZIP |
|
|
|
|
Medical Professional’s Signature |
State Professional License Number (NOT NPI#) |
Today’s Date |
|
|
|
Signature of Collaborating/ Supervising Physician (if signed above by resident/assistant) |
Supervising State Professional License Number |
|
|
|
|
Part 4: Medical Eligibility for
The
Economic need is not a consideration for
The applicant is eligible for
Check all that apply:
NCannot manage, manipulate or insert coins, or obtain tickets in parking meters/ticket machines due to lack of fine motor control of BOTH hands.
NCannot reach above his/her head to a height of 42 inches from the ground due to a lack of finger, hand or
NCannot approach a parking meter due to his/her use of a wheelchair or other device for mobility.
NCannot walk more than 20 feet due to an orthopedic, neurological, cardiovascular or lung condition in which the degree of debilitation is so severe that it almost completely impedes the ability to walk.
NMissing a hand(s) or arm(s) or has permanently lost the use of a hand or arm.
NPatient is under 18 years of age and incapable of driving.
Medical Professional’s Signature
State Professional License Number (NOT NPI#)
Today’s Date
Signature of Collaborating/ Supervising Physician (if signed above by resident/assistant)
Supervising State Professional License Number
FOR SECRETARY OF STATE OFFICE USE ONLY
Parking Placard Number: ________________________________ |
Expiration Date: ______________________________________ |
Issued By: ___________________________________________ |
Issue Date: __________________________________________ |
Document Breakdown
| Fact Name | Details |
|---|---|
| Governing Law | This form is governed by the Illinois Compiled Statutes, specifically 625 ILCS 5/1-159.1. |
| Purpose | The Illinois Placard form is used to apply for a parking placard for individuals with disabilities. |
| Validity Period | A Temporary Placard is valid for three months, while a Permanent Placard lasts for six months from the physician's signature date. |
| Application Types | Applicants can submit for a new placard or request a renewal of an existing one. |
| Minor Applicants | If the applicant is a minor, a parent or legal guardian must also complete a section of the form. |
| Medical Certification | A licensed medical professional must certify the applicant's disability to qualify for the placard. |
| Signature Requirement | Both the applicant and, if applicable, their parent or guardian must sign the form to validate the application. |
| Misuse Consequences | Misuse of the placard can lead to revocation, fines up to $1,000, and possible suspension of the driver's license. |
| Application Submission | Temporary placard applications can be submitted in person or by mail, while Permanent applications must be mailed. |
| Meter-Exempt Parking | Additional certification is required for applicants seeking meter-exempt parking privileges. |
Create More PDFs
Illinois Sales Tax on Cars Bought Out of State - Essential for making necessary corrections to vehicle use tax payments and records in Illinois.
Residential Purchase Agreement - It mandates the seller to provide a current plat of survey and ensure the title's integrity through an owner's title insurance policy.
To ensure clarity and prevent disputes during the dissolution of marriage, utilizing the California Divorce Settlement Agreement form is crucial. This comprehensive legal document helps delineate the distribution of assets, liabilities, child custody details, and more, fundamental for a seamless divorce process. For those looking for an efficient way to handle these arrangements, you can find the necessary resources at California Templates.
Illinois Department of Financial and Professional Regulation - Designed for a broad array of professionals under the Private Detective, Private Alarm, Private Security, Fingerprint Vendor, and Locksmith Act, the form ensures industry-wide standards.