Fill a Valid Illinois Pre Participation Physical Form
Participating in sports is an exciting and rewarding experience for many young athletes in Illinois, but it is crucial to ensure their health and safety before they hit the field or court. The Illinois Pre Participation Physical form is designed to gather essential information about a student's medical history, current health status, and any potential risks associated with athletic participation. This comprehensive form requires input from both the athlete and their parent or guardian, covering various aspects such as medications, allergies, and previous medical conditions. It includes questions about heart health, bone and joint injuries, and other medical concerns that could impact an athlete's ability to compete safely. Additionally, the form addresses specific considerations for female athletes and outlines the necessary physical examination that must be completed by a qualified healthcare provider. By thoroughly completing this form, families can help ensure that young athletes are ready to participate in sports while minimizing the risk of injury or health complications.
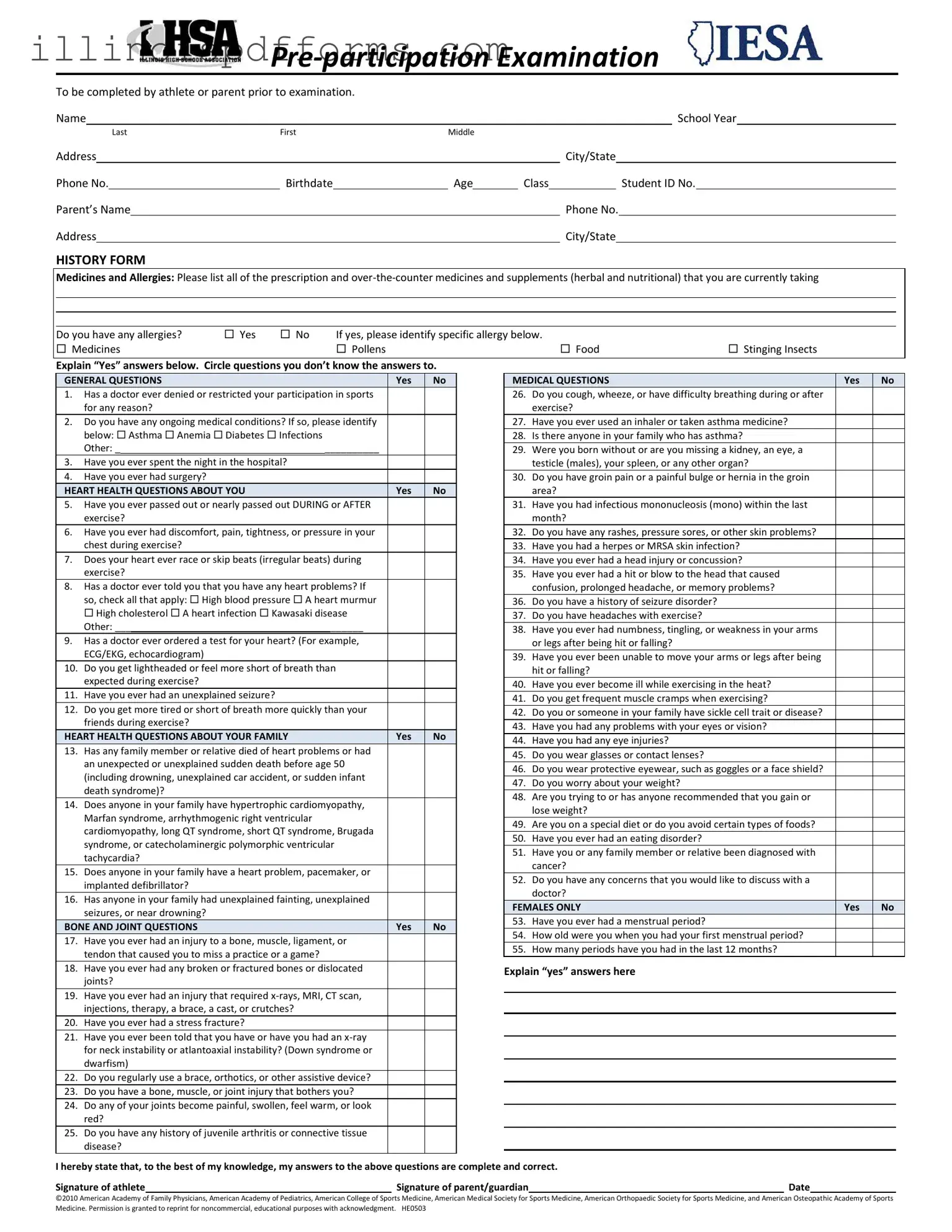
Example - Illinois Pre Participation Physical Form
To be completed by athlete or parent prior to examination. |
|
|
|
|
|
|
|
|
|
|
||||||
Name |
|
|
|
|
|
|
|
|
|
School Year |
||||||
|
|
|
Last |
First |
Middle |
|
|
|
|
|
|
|
|
|||
Address |
|
|
|
|
|
|
|
City/State |
|
|||||||
Phone No. |
|
Birthdate |
|
Age |
Class |
|
|
Student ID No. |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Pare t’s Na e |
|
|
|
|
|
|
Phone No. |
|||||||||
Address |
|
|
|
|
|
|
|
|
City/State |
|
|
|||||
HISTORY FORM
Medicines and Allergies: Please list all of the prescription and
Do you have any allergies? |
Yes |
No |
If yes, please identify specific allergy below. |
|
|
Medicines |
|
|
Pollens |
Food |
Stinging Insects |
|
|
|
|
||
E plain Yes answe s elow. Ci |
le uestions ou don’t know the answe s to. |
|
|
||
|
GENERAL QUESTIONS |
|
|
|
Yes |
No |
|||
1. |
Has a doctor ever denied or restricted your participation in sports |
|
|
||||||
|
|
for any reason? |
|
|
|
|
|
||
2. |
Do you have any ongoing medical conditions? If so, please identify |
|
|
||||||
|
|
below: Asthma Anemia Diabetes Infections |
|
|
|
|
|
||
|
|
Other: _ |
|
__________ |
|
|
|
||
|
|
|
|
|
|
|
|
||
3. |
Have you ever spent the night in the hospital? |
|
|
|
|
|
|||
4. |
Have you ever had surgery? |
|
|
|
|
|
|||
|
HEART HEALTH QUESTIONS ABOUT YOU |
|
|
|
Yes |
No |
|||
5. |
Have you ever passed out or nearly passed out DURING or AFTER |
|
|
||||||
|
|
exercise? |
|
|
|
|
|
||
6. |
Have you ever had discomfort, pain, tightness, or pressure in your |
|
|
||||||
|
|
chest during exercise? |
|
|
|
|
|
||
7. |
Does your heart ever race or skip beats (irregular beats) during |
|
|
||||||
|
|
exercise? |
|
|
|
|
|
||
8. |
Has a doctor ever told you that you have any heart problems? If |
|
|
||||||
|
|
so, check all that apply: High blood pressure A heart murmur |
|
|
|||||
|
|
High cholesterol A heart infection Kawasaki disease |
|
|
|||||
|
|
Other: ___ |
|
|
______ |
|
|
|
|
|
|
|
|
||||||
9. |
Has a doctor ever ordered a test for your heart? (For example, |
|
|
||||||
|
|
ECG/EKG, echocardiogram) |
|
|
|
|
|
||
10. |
Do you get lightheaded or feel more short of breath than |
|
|
||||||
|
|
expected during exercise? |
|
|
|
|
|
||
11. |
Have you ever had an unexplained seizure? |
|
|
|
|
|
|||
12. |
Do you get more tired or short of breath more quickly than your |
|
|
||||||
|
|
friends during exercise? |
|
|
|
|
|
||
|
HEART HEALTH QUESTIONS ABOUT YOUR FAMILY |
|
|
|
Yes |
No |
|||
13. |
Has any family member or relative died of heart problems or had |
|
|
||||||
|
|
an unexpected or unexplained sudden death before age 50 |
|
|
|||||
|
|
(including drowning, unexplained car accident, or sudden infant |
|
|
|||||
|
|
death syndrome)? |
|
|
|
|
|
||
14. |
Does anyone in your family have hypertrophic cardiomyopathy, |
|
|
||||||
|
|
Marfan syndrome, arrhythmogenic right ventricular |
|
|
|
|
|
||
|
|
cardiomyopathy, long QT syndrome, short QT syndrome, Brugada |
|
|
|||||
|
|
syndrome, or catecholaminergic polymorphic ventricular |
|
|
|||||
|
|
tachycardia? |
|
|
|
|
|
||
15. |
Does anyone in your family have a heart problem, pacemaker, or |
|
|
||||||
|
|
implanted defibrillator? |
|
|
|
|
|
||
16. |
Has anyone in your family had unexplained fainting, unexplained |
|
|
||||||
|
|
seizures, or near drowning? |
|
|
|
|
|
||
|
BONE AND JOINT QUESTIONS |
|
|
|
Yes |
No |
|||
17. |
Have you ever had an injury to a bone, muscle, ligament, or |
|
|
||||||
|
|
tendon that caused you to miss a practice or a game? |
|
|
|
|
|
||
18. |
Have you ever had any broken or fractured bones or dislocated |
|
|
||||||
|
|
joints? |
|
|
|
|
|
||
19. |
Have you ever had an injury that required |
|
|
||||||
|
|
injections, therapy, a brace, a cast, or crutches? |
|
|
|
|
|
||
20. |
Have you ever had a stress fracture? |
|
|
|
|
|
|||
21. |
Have you ever been told that you have or have you had an |
|
|
||||||
|
|
for neck instability or atlantoaxial instability? (Down syndrome or |
|
|
|||||
|
|
dwarfism) |
|
|
|
|
|
||
22. |
Do you regularly use a brace, orthotics, or other assistive device? |
|
|
||||||
23. |
Do you have a bone, muscle, or joint injury that bothers you? |
|
|
||||||
24. |
Do any of your joints become painful, swollen, feel warm, or look |
|
|
||||||
|
|
red? |
|
|
|
|
|
||
25. |
Do you have any history of juvenile arthritis or connective tissue |
|
|
||||||
|
|
disease? |
|
|
|
|
|
||
MEDICAL QUESTIONS |
Yes |
No |
26.Do you cough, wheeze, or have difficulty breathing during or after exercise?
27. |
Have you ever used an inhaler or taken asthma medicine? |
|
|
28. |
Is there anyone in your family who has asthma? |
|
|
29. |
Were you born without or are you missing a kidney, an eye, a |
|
|
|
testicle (males), your spleen, or any other organ? |
|
|
30. |
Do you have groin pain or a painful bulge or hernia in the groin |
|
|
|
area? |
|
|
31. |
Have you had infectious mononucleosis (mono) within the last |
|
|
|
month? |
|
|
32. |
Do you have any rashes, pressure sores, or other skin problems? |
|
|
33. |
Have you had a herpes or MRSA skin infection? |
|
|
34. |
Have you ever had a head injury or concussion? |
|
|
35. |
Have you ever had a hit or blow to the head that caused |
|
|
|
confusion, prolonged headache, or memory problems? |
|
|
36. |
Do you have a history of seizure disorder? |
|
|
37. |
Do you have headaches with exercise? |
|
|
38. |
Have you ever had numbness, tingling, or weakness in your arms |
|
|
|
or legs after being hit or falling? |
|
|
39. |
Have you ever been unable to move your arms or legs after being |
|
|
|
hit or falling? |
|
|
40. |
Have you ever become ill while exercising in the heat? |
|
|
41. |
Do you get frequent muscle cramps when exercising? |
|
|
42. |
Do you or someone in your family have sickle cell trait or disease? |
|
|
43. |
Have you had any problems with your eyes or vision? |
|
|
44. |
Have you had any eye injuries? |
|
|
45. |
Do you wear glasses or contact lenses? |
|
|
46. |
Do you wear protective eyewear, such as goggles or a face shield? |
|
|
47. |
Do you worry about your weight? |
|
|
48. |
Are you trying to or has anyone recommended that you gain or |
|
|
|
lose weight? |
|
|
49. |
Are you on a special diet or do you avoid certain types of foods? |
|
|
50. |
Have you ever had an eating disorder? |
|
|
51. |
Have you or any family member or relative been diagnosed with |
|
|
|
cancer? |
|
|
52. |
Do you have any concerns that you would like to discuss with a |
|
|
|
doctor? |
|
|
FEMALES ONLY |
Yes |
No |
|
53. |
Have you ever had a menstrual period? |
|
|
54.How old were you when you had your first menstrual period?
55.How many periods have you had in the last 12 months?
Explain es answe s he e
I hereby state that, to the best of my knowledge, my answers to the above questions are complete and correct.
Signature of athlete |
|
Signature of parent/guardian |
|
Date |
©2010 American Academy of Family Physicians, American Academy of Pediatrics, American College of Sports Medicine, American Medical Society for Sports Medicine, American Orthopaedic Society for Sports Medicine, and American Osteopathic Academy of Sports Medicine. Permission is granted to reprint for noncommercial, educational purposes with acknowledgment. HE0503
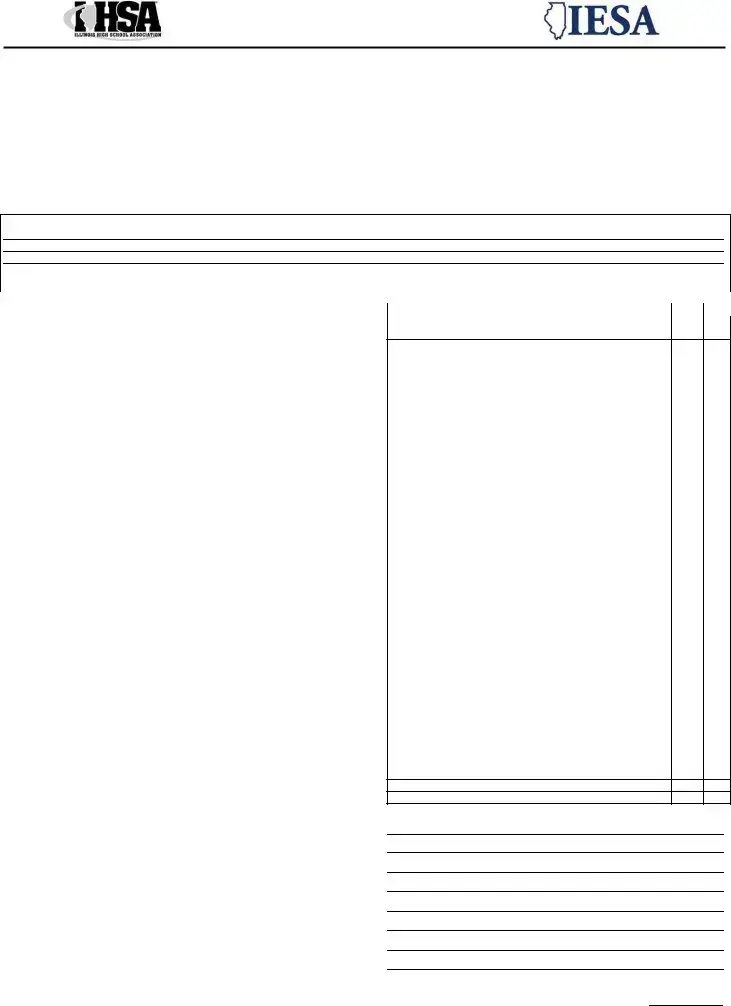
PHYSICAL EXAMINATION FORM
|
EXAMINATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Height |
|
|
Weight |
|
Male |
Female |
|
|
|
|
|
|
|
||
|
BP |
/ |
( |
/ |
) |
Pulse |
Vision R 20/ |
L 20/ |
|
|
Corrected |
Y N |
||||
|
MEDICAL |
|
|
|
|
|
|
|
NORMAL |
|
|
ABNORMAL FINDINGS |
|
|
||
|
Appearance |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• Marfan stigmata (kyphoscoliosis, |
|
|
|
|
|
|
|
|
|
||||||
|
arachnodactyly, arm span > height, hyperlaxity, myopia, MVP, aortic insufficiency) |
|
|
|
|
|
|
|
|
|||||||
|
Eyes/ears/nose/throat |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Pupils equal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hearing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lymph nodes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Heart a |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Murmurs (auscultation standing, supine, +/- Valsalva) |
|
|
|
|
|
|
|
|
|
|
|||||
|
Location of point of maximal impulse (PMI) |
|
|
|
|
|
|
|
|
|
|
|||||
|
Pulses |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Simultaneous femoral and radial pulses |
|
|
|
|
|
|
|
|
|
|
|||||
|
Lungs |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Abdomen |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Genitourinary (males only)b |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Skin |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HSV, lesions suggestive of MRSA, tinea corporis |
|
|
|
|
|
|
|
|
|
|
|||||
|
Neurologic c |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MUSCULOSKELETAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Neck |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Back |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Shoulder/arm |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Elbow/forearm |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Wrist/hand/fingers |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hip/thigh |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Knee |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Leg/Ankle |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Foot/toes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Functional |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
aConsider ECG, echocardiogram, and referral to cardiology for abnormal cardiac history or exam. |
|
|
|
|
|
|
|
|
|
|||||||
bConsider GU exam if in private setting. Having third party present is recommended. |
|
|
|
|
|
|
|
|
|
|||||||
cConsider cognitive evaluation or baseline neuropsychiatric testing if a history of significant concussion. |
|
|
|
|
|
|
|
|
|
|||||||
O the |
asis of the e a i |
atio |
o this da |
, I appro e this |
hild’s parti ipatio i |
i ters holasti |
sports for o |
e year. |
|
|
||||||
Yes |
|
|
|
No |
|
Limited |
|
|
|
|
|
Examination Date |
|
|
||
Additional Comments:
Ph |
si ia |
’s Sig ature |
|
Ph |
si ia |
’s Assista t Sig ature* |
|
Ad a ed Nurse Pra titio er’s Sig ature* |
|
||
*effective January 2003, the IHSA Board of Dire tors appro ed a re o |
e datio , o siste t ith the Illi ois S hool Code, that allo s Ph si ia ’s Assista ts or |
||
Advanced Nurse Practitioners to sign off on physicals. |
|
||
IHSA Steroid Testing Policy Consent to Random Testing
(This section for high school students only)
As a prerequisite to participation in IHSA athletic activities, we agree that I/our student will not use
day, and I/our student do/does hereby agree to submit to such testing and analysis by a certified laboratory. We further understand and agree that the results of the
A complete list of the current IHSA Banned Substance Classes can be accessed at
http://www.ihsa.org/initiatives/sportsMedicine/files/IHSA_banned_substance_classes.pdf
|
|
|
|
|
|
|
|
|
|
Signature of |
|
Date |
|
Signature of |
|
Date |
|
Document Breakdown
| Fact Name | Detail |
|---|---|
| Purpose of the Form | The Illinois Pre Participation Physical form is designed to assess an athlete's health and fitness before participating in sports. |
| Governing Laws | This form is governed by the Illinois School Code, particularly Section 27-23.1, which mandates physical examinations for student athletes. |
| Completion Requirement | The form must be completed by the athlete or their parent before the physical examination takes place. |
| Medical History | A comprehensive medical history is required, including any ongoing medical conditions, allergies, and previous injuries. |
| Heart Health Questions | Specific questions regarding heart health are included to identify potential risks associated with athletic participation. |
| Bone and Joint Questions | The form contains inquiries about previous bone or joint injuries, ensuring that any past issues are documented. |
| Signature Requirement | Both the athlete and a parent or guardian must sign the form, affirming the accuracy of the provided information. |
| Confidentiality | Results from any performance-enhancing substance testing will be kept confidential in accordance with applicable laws. |
Create More PDFs
Illinois School Physical Form 2022 - System reviews cover various bodily systems and conditions, requiring comments or follow-up actions if necessary.
In addition to understanding the importance of the California Motorcycle Bill of Sale, it is helpful to refer to resources that provide templates and guidance for this process. For more information and a convenient template, you can visit templates-guide.com/california-motorcycle-bill-of-sale-template, which offers valuable insights for both buyers and sellers.
Foid Card Application Chicago - The return process for the firearm control card upon termination of an employee's position involves specific steps to ensure accountability and compliance.
Application for Waiver of Court Fees and Costs - Ensuring accuracy and completeness of the application details facilitates a smoother review process by the Illinois Department of Public Health.