Fill a Valid Illinois Wage Verification Form
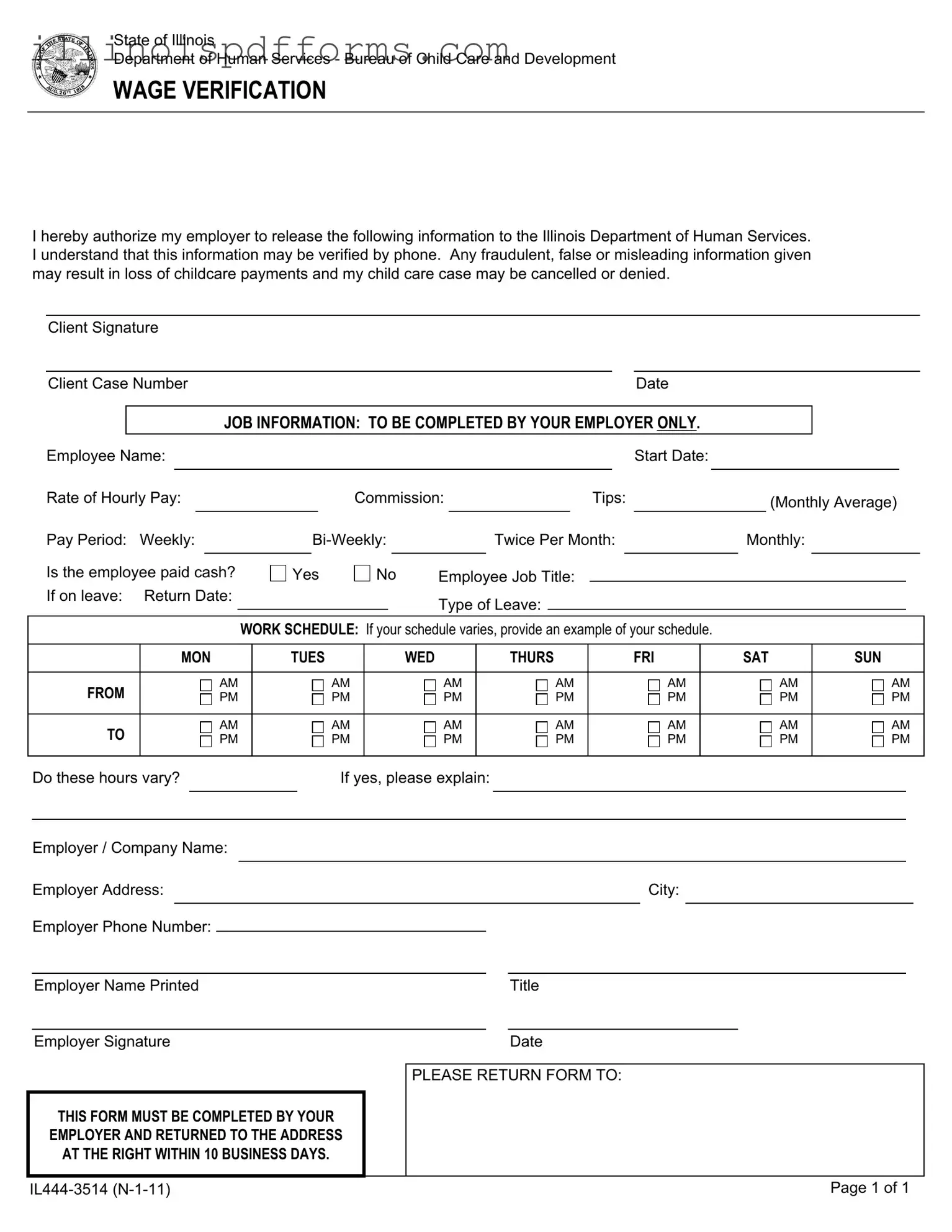
The Illinois Wage Verification form plays a crucial role in the state's childcare assistance program by ensuring that the income of applicants is accurately documented. This form is designed to facilitate communication between employees and their employers, allowing necessary wage information to be shared with the Illinois Department of Human Services. By signing the form, employees authorize their employers to disclose details such as hourly pay rates, commission, and tips, which are vital for determining eligibility for childcare benefits. Employers are responsible for filling out specific sections, including job title, work schedule, and whether the employee is paid in cash. The form also emphasizes the importance of providing truthful information, as any fraudulent claims could lead to serious consequences, including the loss of childcare payments or denial of the application. Timeliness is critical; employers must return the completed form within ten business days to ensure the application process continues smoothly. This form ultimately aims to protect both the employee's rights and the integrity of the childcare assistance program.
Example - Illinois Wage Verification Form
State of Illinois
Department of Human Services - Bureau of Child Care and Development
WAGE VERIFICATION
I hereby authorize my employer to release the following information to the Illinois Department of Human Services. I understand that this information may be verified by phone. Any fraudulent, false or misleading information given may result in loss of childcare payments and my child care case may be cancelled or denied.
Client Signature
Client Case NumberDate
JOB INFORMATION: TO BE COMPLETED BY YOUR EMPLOYER ONLY.
Employee Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Start Date: |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Rate of Hourly Pay: |
|
|
|
|
|
Commission: |
|
|
|
|
Tips: |
|
|
(Monthly Average) |
|
||||||||||||||||
Pay Period: |
Weekly: |
|
|
|
|
|
Twice Per Month: |
Monthly: |
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Is the employee paid cash? |
|
Yes |
|
No |
Employee Job Title: |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
If on leave: |
Return Date: |
|
|
|
|
|
|
|
|
Type of Leave: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
WORK SCHEDULE: If your schedule varies, provide an example of your schedule. |
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
MON |
|
TUES |
|
|
|
|
WED |
|
THURS |
|
|
FRI |
|
SAT |
SUN |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
FROM |
|
|
|
AM |
|
|
|
|
AM |
|
AM |
|
|
AM |
|
|
|
AM |
|
|
AM |
AM |
|
||||||||
|
|
|
PM |
|
|
|
|
PM |
|
PM |
|
|
PM |
|
|
|
PM |
|
|
PM |
PM |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
TO |
|
|
|
AM |
|
|
|
|
AM |
|
AM |
|
|
AM |
|
|
|
AM |
|
|
AM |
AM |
|
||||||||
|
|
|
PM |
|
|
|
|
PM |
|
PM |
|
|
PM |
|
|
|
PM |
|
|
PM |
PM |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Do these hours vary? |
If yes, please explain: |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer / Company Name: |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer Address: |
|
|
|
|
|
City: |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Employer Phone Number: |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
||||||
Employer Name Printed |
|
|
|
|
Title |
|
|
|||||||
|
|
|
|
|
|
|
|
|
||||||
Employer Signature |
|
|
|
|
Date |
|
|
|||||||
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
PLEASE RETURN FORM TO: |
|
|
||||||
THIS FORM MUST BE COMPLETED BY YOUR
EMPLOYER AND RETURNED TO THE ADDRESS
AT THE RIGHT WITHIN 10 BUSINESS DAYS.
Page 1 of 1 |
Document Breakdown
| Fact Name | Description |
|---|---|
| Purpose of the Form | The Illinois Wage Verification form is designed to authorize employers to provide necessary wage information to the Illinois Department of Human Services for childcare assistance programs. |
| Governing Law | This form is governed by the Illinois Child Care Assistance Program (CCAP) regulations, which ensure that families receive appropriate financial support for childcare based on their income. |
| Employer's Responsibility | Employers must complete the form accurately and return it to the specified address within 10 business days to avoid delays in childcare payments. |
| Consequences of Misrepresentation | Providing false or misleading information on this form can lead to severe consequences, including the potential loss of childcare payments and cancellation of the childcare case. |
Create More PDFs
2024 Illinois Turkey Season Dates - Group hunts are facilitated through the application process, with the option to apply for permits together in the first two lotteries.
When considering the importance of a California Power of Attorney form, it's essential to understand the complexities involved in designating a trusted individual for your financial or medical decisions. You can find a useful resource to help you navigate this process at https://templates-guide.com/california-power-of-attorney-template, ensuring that your wishes are effectively represented and your affairs are managed appropriately in times of need.
How to Get a Sponsoring Broker for Real Estate - A fundamental document for those in the Illinois real estate industry to comply with state licensing requirements.